













 6 / 22
6 / 22

2017 EXPAT BENEFITS
GUIDE
4
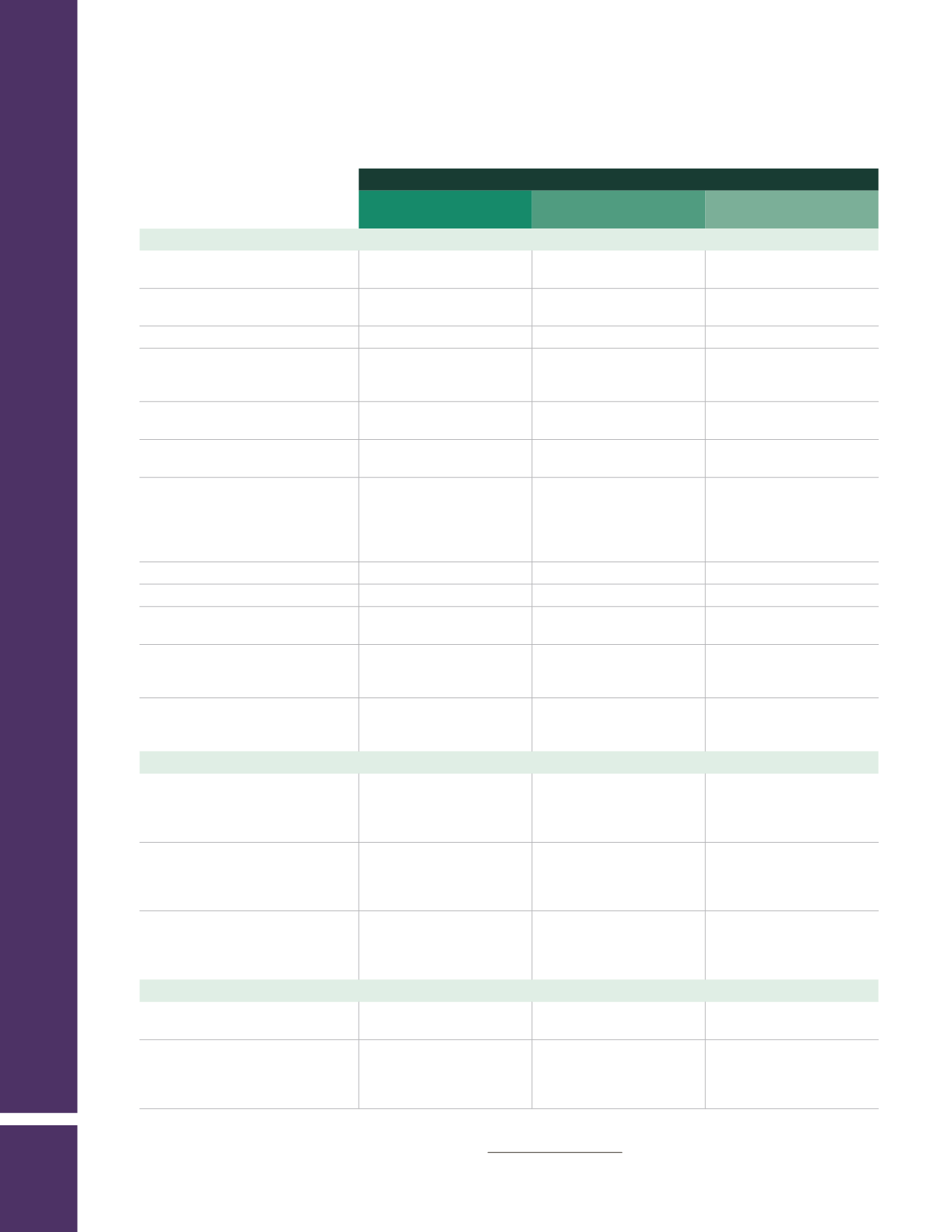
AETNA INTERNATIONAL — Medical Benefits
Outside the U.S.
In-Network**
(Inside the U.S.)
Out-of-Network
(Inside the U.S.)
Other Services
Skilled nursing facility
(120-day calendar year maximum)
90%*
80%
60% after $250 per
confinement deductible
Hospice care facility inpatient
90%*
80%
60% after $250 per
confinement deductible
Hospice care facility outpatient
90%*
80%
60% after deductible
Home health care
(120-visit calendar year maximum,
includes Private Duty Nursing)
90%*
80%
60% after deductible
Spinal disorder treatment
($1,000 per calendar year maximum)
90%*
80%
60% after deductible
Short-term rehabilitation
(60 visits per calendar year maximum)
90%*
80%
60% after deductible
Autism treatment
(inpatient/outpatient
services, medication management and
diagnostic services; speech therapy
with 60 visits per calendar year
maximum)
90%*
80%
60% after deductible
Diagnostic outpatient lab and X-ray
90%*
80%
60% after deductible
Bariatric surgery
90%*
80%
60% after deductible
Durable medical equipment
(including foot orthotics)
90%*
80%
60% after deductible
Hearing aids
(maximum benefit of $3,000 every
36 months)
90%*
80%
60% after deductible
Global emergency assistance program
($500,000 per calendar year
maximum)
100%
100%
100%
Prescription Drug Coverage
Generic
(365-day maximum supply)
75%*
75%, member cost not to
exceed $50 per 30-day
supply (includes
Mail-Order Drugs)
60% after deductible
Preferred brand
(365-day maximum supply)
75%*
75%, member cost not to
exceed $100 per 30-day
supply (includes
Mail-Order Drugs)
60% after deductible
Non-preferred brand
(365-day maximum supply)
75%*
75%, member cost not to
exceed $125 per 30-day
supply (includes
Mail-Order Drugs)
60% after deductible
Vision Expenses
Routine eye exam
(One exam every 12 months)
90%*
100%
60% after deductible
Eyeglass frames and lenses OR
contact lenses
(One frames/lenses or
contacts per 12 months)
90% after $35 copay
80% after $35 copay
60% after $35 copay
* The plan pays 100% for covered services outside the U.S. for employees enrolled in the Saudi Arabia or other Middle East Plans.
** To find a participating in-network provider in the U.S., log on to
www.aetnanavigator.comor call the International Member Service
Center at 1-800-231-7729 or 1-813-775-0190 (collect calls are accepted).